Cleft Lip & Palate - Pediatric

Cleft lip and palate is one of the most common birth defects in the United States. The defect occurs when either the lip or the palate (roof of the mouth), or both, do not join together properly during development. With the use of prenatal screening such as ultrasounds, this can frequently be recognized and diagnosed before birth.
ACPA Approved Team

UK Pediatric Plastic Surgery Clinic is an ACPA Approved Team and has met the Standards of Team Care for Cleft and Craniofacial Teams set by the American Cleft Palate Craniofacial Association (ACPA). The ACPA Commission on the Approval of Teams has determined that UK Pediatric Plastic Surgery Clinic is capable of providing cleft and craniofacial care in a coordinated and consistent manner, that care provided by UK Pediatric Plastic Surgery Clinic follows the proper sequence and takes place within the framework of the patient’s overall developmental, medical and psychological needs. All approved teams in the U.S. and Canada are listed on the ACPA website.
Treatment
Cleft lip and palate are corrected at separate times, and this can vary from surgeon to surgeon. At UK, we aim to fix the lip at 2-3 months of age, although this can be done later depending on how the child’s weight gain and growth are progressing.
Lip surgery can be done on an outpatient basis; however, this is best discussed with the cleft surgeon.
The palate is usually fixed when a child is 6 months to a year old, depending on the type of cleft and the child’s general state of health. Palate surgery usually requires an overnight stay and, depending on how well the patient is eating and drinking, he or she can usually go home the next day. We encourage an applesauce consistency diet (Stage 2 baby food). Both lip and palate surgeries require children to wear arm restraints (No-Nos) which keep them from putting their fingers or other hard objects in their newly repaired mouths.
After lip and/or palate surgery, routine clinic visits will ensure that the child is doing well with both eating and speech. As children enter into kindergarten, it is not uncommon to “touch up” their lip repair to reduce any unnecessary attention from other children. The patient will also have comprehensive speech evaluations to ensure the palate is working properly.
See the cleft palate guideline (link below) for suggested timing of procedures.
For more information about cleft lip and palate, please refer to the American Society of Plastic Surgeons website.
UK pediatric plastic surgeons are dedicated to providing the best cleft care to your child.
NOTE: The previous descriptions and notes are intended to give an overview and are not at all comprehensive. Should you have any questions or concerns, please do not hesitate to contact UK Pediatric Plastic Surgery for a clinic consultation.
What does it look like?
Cleft lip can either occur on one side of the mouth or both sides. Cleft palates can also be located on either one or both sides of the mouth, as well as only the soft part of the palate. Because fusion of different parts of the face, mouth and palate takes place at different times during development, a wide variety of lip and palate clefts can occur.
Clefts can involve more than merely the lip or palate. In extreme cases a severe midline cleft palate may involve the entire face. Read about one such case treated by UK HealthCare's Dr. James Liau.
Cleft lip
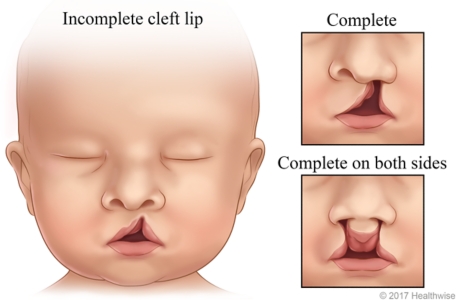
Cleft lip is a birth defect that occurs when the tissues of the upper jaw and nose do not join as expected during fetal development, resulting in a split (cleft) in the lip. An incomplete cleft lip can range from a slight indentation to a notch in the upper lip on one or both sides. A complete cleft lip is a deep split in the lip that extends into one or both sides of the nose. Cleft lip can be corrected with one or more surgeries.
How does it affect my child?
Cleft lip can greatly affect a child’s overall appearance, and total correction is the ultimate goal. Depending on the severity of the cleft, the nose may also be involved in the treatment process. The goal of cleft lip correction is to make both sides of the mouth look the same, resulting in an appearance that is as close to normal as possible.
Cleft palate might or might not exist alongside a cleft lip. Either way, the palate serves to keep the nose space separate from the mouth. If this barrier does not exist, several difficulties might arise. Food and liquid can easily pass from the mouth into the nose, making it difficult for the child to drink and/or eat. Special bottles and nutritional therapists can help with newborns learning to eat.
As the child grows older, speech can become a major concern, as many sounds cannot form in the mouth without the aid of a palate.
Related conditions
Another issue that can accompany cleft palates involves the palatal muscles, which help open the middle ear. When a cleft palate occurs, the middle ears might not empty as normal, resulting in repeated ear infections. Ear tubes are regularly used in these cases, and they can be inserted on the day of the palate surgery. Hearing can also be affected and must be checked routinely.
There is also a type of cleft palate called a submucous cleft, which occurs when the palate appears intact but there are muscular problems beneath the skin on the inside of the mouth. Diagnosis can be based on three separate areas of the mouth: 1) cleft or bifid uvula (the “punching bag” hanging down from the roof of the mouth); 2) zona pellucidum (a thin, whitish line going down the middle of the palate); and 3) a notch in the back of the hard palate (which can only be felt during an exam). The concerns for a submucous cleft are similar to those regarding speech and middle-ear infections.

